Quick answer: CGM and fingerstick readings often differ because they measure glucose in different places. One reads your blood directly, the other reads the fluid between your cells. Those two values don't always agree in real time, and most of the time there's a simple explanation.
Your fingerstick shows 142 mg/dL. Your CGM says 168. You check again. Still off.
Neither device is necessarily broken. They just measure different things, in different places, at slightly different times. Once you understand why that happens, a mismatch stops being scary and starts being useful information.
Why They Don't Always Match
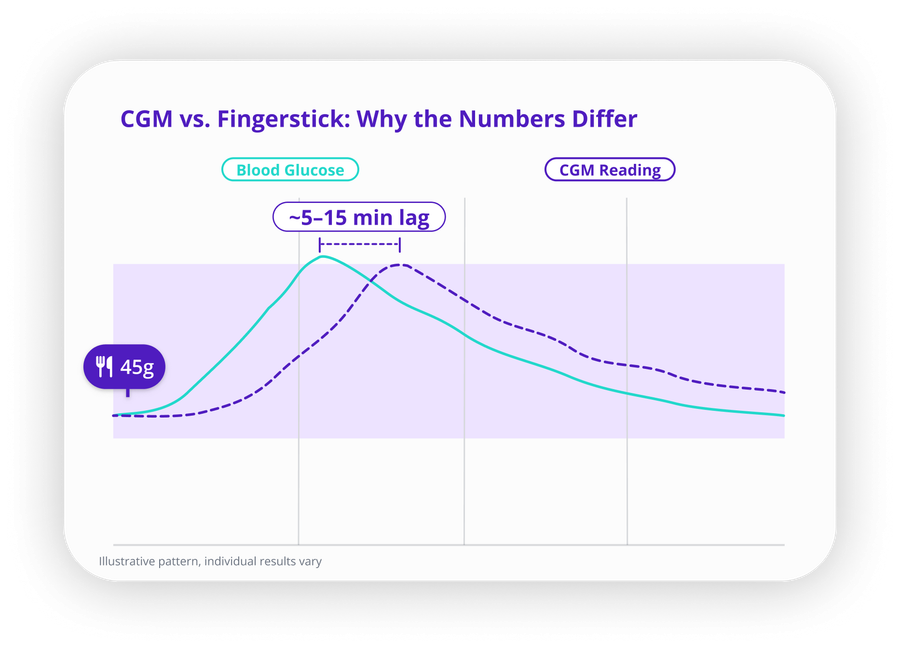
CGMs measure glucose in interstitial fluid, which is the fluid that surrounds your cells just beneath the skin. A fingerstick meter measures glucose directly from your blood. Under stable conditions these two values track closely. But they are not the same measurement, and that gap matters most when your glucose is moving fast.
6 Reasons Your CGM and Fingerstick Don't Agree
1. Your Glucose Is Moving and the CGM Is Catching Up
This is the most common reason, and it explains a lot. Interstitial glucose lags behind blood glucose by roughly 5 to 15 minutes. So when you're rising after a meal or dropping after a correction, the CGM is showing you where you were a few minutes ago, not where you are right now.
Your fingerstick reads the present. Your CGM reads the recent past. During rapid swings, that gap is noticeable.
2. The Sensor Is Still Warming Up
A new sensor needs time to settle. Depending on which CGM you use, that warm-up window can stretch anywhere from a couple of hours to most of a day. During that time the readings are less reliable, and discrepancies are common.
If your numbers look off right after a sensor change, this is usually why. Give it time before you start second-guessing the device.
3. You Slept on the Sensor
Lying on your sensor compresses the tissue around it and temporarily restricts the interstitial fluid the CGM needs to read accurately. The result is a falsely low reading, sometimes dramatically low, while you're sleeping.
If you wake up to a low alert but feel completely fine and your fingerstick is normal, that's almost certainly a compression low and not a real drop. For more on this, see why your CGM shows false lows and how to fix them.
4. The Calibration Got Corrupted
Some CGMs let you calibrate manually with a fingerstick reading. That's useful when done right, but if you calibrate while your glucose is actively rising or falling, or if the fingerstick itself was off because of unwashed hands, a squeezed fingertip, or an old test strip, the CGM can lock in that error and carry it forward.
Calibrate only when things are stable. Stable glucose, clean hands, fresh strip.
5. You Just Ate Something That Spiked Fast
A high-carb meal can push blood glucose up sharply in a short window. During the steepest part of that rise, the lag between blood and interstitial glucose is at its most visible. Your fingerstick catches the spike first. Your CGM follows a few minutes later.
This isn't a malfunction. It's physics. For help making sense of what your CGM graph looks like after eating, see normal CGM graph after eating: what patterns are common.
6. Something in the Environment Is Affecting the Sensor
Heat, cold, dehydration, certain medications (acetaminophen is the most well-known example for older sensors), reduced blood flow at the insertion site, and sensors that are near the end of their approved wear time can all nudge readings off.
If your CGM is consistently reading high or low compared to multiple stable fingerstick checks over a day or two, contact the manufacturer. Sensor defects happen, and most companies will replace them without much pushback.
What to Do When the Numbers Don't Match
Start simple. Check the trend arrow on your CGM. A flat arrow and a small gap between devices is usually nothing. A steep arrow during a mismatch almost always means lag, not error.
If the gap is more than 20 to 30 mg/dL and your trend looks stable, run through this before drawing conclusions.
Wash your hands and retest. Dirty hands, residue from food, and squeezing the fingertip too hard can all throw off a fingerstick reading. A clean retest with a fresh strip fixes more mismatches than people expect.
Look at the timing. Did you eat recently? Take a correction? Exercise? All of these create rapid glucose movement, and rapid movement is when CGM lag shows up most clearly. Wait until things settle and check again.
Check the sensor. How old is it? Has it been under pressure? A sensor in its final days or one that's been getting compressed at night is more likely to drift.
If mismatches keep happening across stable periods with no obvious trigger, replace the sensor and reach out to the manufacturer if it continues.
When You Should Still Use a Fingerstick
CGMs are not approved as a standalone replacement for fingerstick testing in every situation. Before treating a suspected low, most manufacturers still recommend confirming with a fingerstick, especially if your symptoms don't line up with what the CGM is showing.
When in doubt and a decision is on the line, the fingerstick is still your most direct read.
How SNAQ Helps You Make Sense of It
A mismatch in isolation tells you almost nothing. The same 30 mg/dL gap means something completely different depending on whether it happened 20 minutes after a big meal, on night three of a sensor's life, or on a Tuesday morning when you hadn't eaten anything.
SNAQ connects your CGM data with your meal logs so you can see the full picture at a glance. When a mismatch shows up, you can actually see what was happening around it, which turns a confusing number into a pattern you can learn from.
That context is what a CGM alone, or a fingerstick alone, can't give you.
References
- American Diabetes Association. Standards of Medical Care in Diabetes 2023. Diabetes Care, 2023.
- Rebrin K, Steil GM. Can Interstitial Glucose Assessment Replace Blood Glucose Measurements? Diabetes Technol Ther, 2022.
- Beck RW, et al. Continuous Glucose Monitoring Versus Self-monitoring in Type 1 Diabetes. N Engl J Med, 2017.
- Klonoff DC. False alarms in continuous glucose monitoring systems. J Diabetes Sci Technol, 2012.