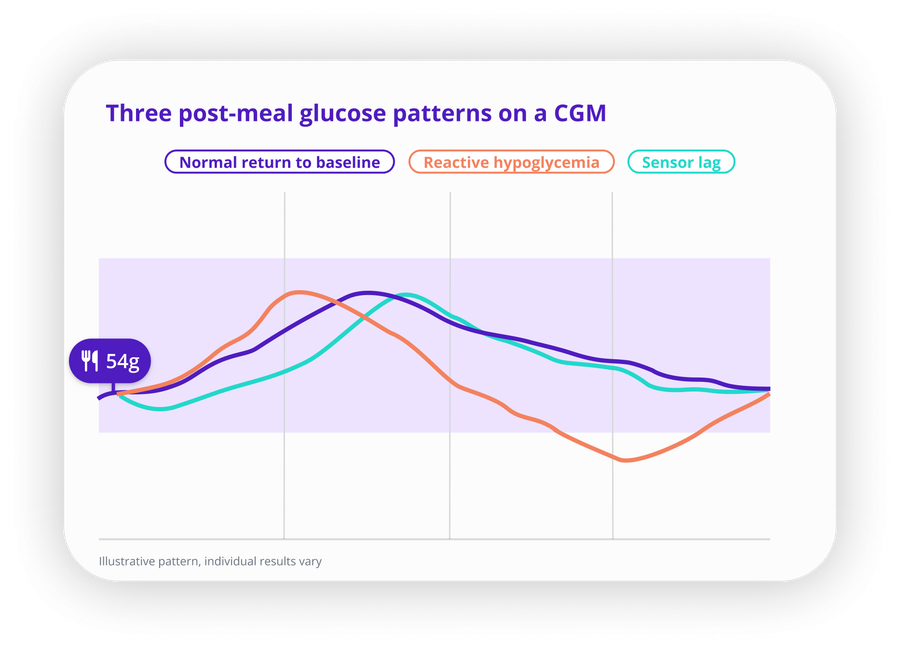
Quick answer: A post-meal dip on your CGM can mean three different things: a normal return to baseline, sensor lag catching up to a glucose change that already happened in your blood, or reactive hypoglycemia driven by an exaggerated insulin response. The curve shape and timing are usually the most useful clues for telling them apart.
A post-meal glucose drop can look alarming on a CGM, especially when you expected the curve to climb. But the same dip shape can come from completely different causes, and reading it correctly changes what you do next. Sensor lag, meal composition, and genuine reactive hypoglycemia can all produce what looks like a drop on screen, and they have little in common beyond the appearance.
Understanding which one you're likely looking at helps you interpret your data more accurately and decide when a dip deserves attention.
What a Normal Post-Meal Glucose Curve Looks Like
In people without diabetes, blood glucose rises after eating, peaks within one to two hours, then returns to baseline without dropping below where it started. The rise is usually modest and the descent is gradual.
In people with diabetes, the shape varies more. You might see a sharper peak, a slower rise, a delayed spike several hours later, or a post-peak drop that goes below your pre-meal level. Not every variation is a problem. But understanding what drives each shape makes the pattern easier to investigate.
If you are newer to reading CGM curves after meals, Normal CGM Graph After Eating: What Patterns Are Common? walks through the most common shapes and what tends to drive them.
Cause 1: Reactive Hypoglycemia
Reactive hypoglycemia happens when the body releases more insulin than needed after a meal, pushing glucose lower than expected. It typically occurs within two to four hours of eating, most often after meals high in refined carbohydrates or simple sugars.
For people with Type 2 diabetes, one pattern that can contribute is when insulin release is delayed. By the time insulin arrives, glucose is already starting to fall from its peak on its own. The delayed surge then pushes it further than expected.
For people with Type 1 diabetes using insulin, a similar drop can happen when the meal turns out to absorb more slowly than expected due to fat, fiber, or a smaller portion than estimated, and insulin activity continues past the carb absorption window.
Signs that point toward reactive hypoglycemia rather than a sensor artifact:
- The dip appears within two to four hours of eating
- You feel shaky, sweaty, dizzy, or unusually hungry
- The drop is steeper and lower than your usual post-meal return to baseline
- The same meal has produced a similar pattern on other days
That last point matters most. A single dip is a data point. A recurring dip after similar meals is a pattern worth discussing with your care team.
Cause 2: CGM Sensor Lag
CGMs measure glucose in the interstitial fluid, the fluid between your cells, not directly in your blood. That reading can lag behind blood glucose by roughly 5 to 15 minutes, and the gap can be wider during rapid glucose changes. Research published by the American Diabetes Association found physiological lag times ranging from 4 to 50 minutes depending on conditions.
After a fast-digesting meal, this lag can create a misleading picture. Blood glucose climbs first. The CGM follows. If you look at your CGM right after eating, the sensor may still show a lower number even though your blood glucose has already been rising for several minutes.
The opposite can also happen. Blood glucose starts to fall while the CGM is still catching up to the peak. The result looks like a sudden post-meal dip on screen, but what you are actually seeing is the sensor tracking a drop that started in the blood a few minutes earlier.
Sensor lag is most noticeable during rapid glucose changes, which is exactly what happens after a fast-digesting meal. If you ate a high-carb meal, moved around, and noticed a brief low reading that self-corrected within one reading or two, lag is a reasonable first explanation to consider.
One other thing worth ruling out, especially during the day: a CGM pressed against a tight waistband, a desk edge, or an armrest during a meal can reduce fluid around the sensor and produce a brief false low. This kind of compression low is more commonly associated with sleep, but it can happen during the day too. A reading that looks like a sharp sudden dip while you were sitting still is worth a fingerstick to confirm.
If you are seeing unexpected lows and want to go deeper on sensor accuracy, Why Your CGM Gives False Lows covers compression lows, sensor placement, and calibration drift in more detail.
Cause 3: How Meal Composition Affects the Curve Shape
What you ate and how quickly it digests shapes the curve more than most people expect.
Protein, fat, and fiber slow absorption
A meal with significant protein, fat, or fiber takes longer to digest. The glucose rise may be smaller, flatter, or delayed. If you check your CGM expecting a spike and see a modest rise that levels off, the meal composition may be doing exactly what it is supposed to do. A prolonged flat stretch after eating is not the same as a dip, even though it can feel that way if your expectation was a visible climb.
High-carb meals and an exaggerated insulin response
Meals high in refined carbohydrates, especially without much protein or fat to slow digestion, can trigger a fast glucose rise. The pace of that rise prompts the pancreas to release insulin. If the insulin response overshoots or the carbs absorb faster than the response anticipated, glucose can fall quickly once absorption is complete.
White bread, sugary drinks, pastries, and fruit juice on an empty stomach are the meals most commonly associated with this pattern. The faster the rise, the sharper the potential drop. Adding protein or fat to the same meal tends to flatten both.
Morning and the dawn phenomenon
If the dip tends to happen after breakfast more than after other meals, morning physiology may be a factor. Many people with diabetes experience some degree of morning insulin resistance driven by hormonal shifts overnight. A breakfast that sits fine at lunch might produce a different curve early in the morning because the body is handling glucose less efficiently at that hour. The same food, a different time of day, can behave meaningfully differently.
Cause 4: Exercise and Stress Around Meal Time
Physical activity is one of the more reliable ways to create a post-meal glucose drop, particularly if you moved around in the one to two hours after eating. Muscles use glucose during activity, which can pull glucose down faster than it would fall at rest. When that overlaps with the natural post-peak descent, the combined effect can look steeper on a CGM than either cause would produce alone.
Stress has a different mechanism. Cortisol and adrenaline can raise glucose temporarily. Once the stress response fades, glucose may fall quickly, and if that happens during the post-meal period, the drop can appear more dramatic than the meal alone would explain.
If you notice frequent post-meal dips on days when you ate at your desk during a stressful meeting, walked home after lunch, or had a harder workout before dinner, the timing may be more relevant than the food itself.
How to Tell if the Dip Deserves Attention
Not every post-meal glucose drop needs action. Here is a practical way to work through what you are seeing.
Check the timing. A dip that appears within two to four hours of eating and comes with symptoms like shakiness, sweating, or confusion points more toward reactive hypoglycemia. A brief dip that appears in the first 30 to 45 minutes after eating and then self-corrects is more consistent with sensor lag.
Look at the curve shape. A smooth, gradual return to your pre-meal level is normal. A sharp V-shaped drop that goes well below where you started, especially if it keeps falling rather than leveling off, is worth a closer look.
Compare the drop to your baseline. A modest drop back toward your pre-meal level is different from a steep drop that goes considerably lower. The steepness and the endpoint both matter.
Confirm with a fingerstick if in doubt. If your CGM shows a low reading and you are not feeling symptoms, a fingerstick glucose test can tell you whether the reading is accurate or a sensor artifact. If the fingerstick agrees with the CGM, the reading is likely real.
Check whether it repeats. A single post-meal dip after an unusual meal is rarely meaningful on its own. The same pattern appearing after similar meals, at similar times, across multiple days is what makes it worth reviewing with your care team.
What to Test If the Dip Keeps Happening
If you are seeing recurring post-meal dips, a few changes are worth testing before drawing conclusions.
Add protein or fat to high-carb meals. Pairing carbs with protein, fat, or fiber slows digestion and tends to blunt both the rise and the following drop. Toast alone behaves differently than toast with eggs or peanut butter.
Test the same meal at different times of day. If breakfast consistently produces a dip that lunch does not, morning insulin sensitivity may be contributing. The same food can behave differently at 7am versus noon.
Review portion size. A larger portion of the same meal triggers a stronger glucose response. Testing a smaller portion on a different day can show whether size is part of the pattern.
Note what you were doing right after eating. A walk, a workout, or even sitting in a compressed position for an extended period can each affect the curve in different ways. Logging activity context alongside the meal makes the pattern easier to read later.
Look across days, not meals. A single dip after a single meal is a starting point, not a conclusion. The question worth asking is whether the same meal, at the same time of day, with similar activity afterward, keeps producing the same shape.
If you use SNAQ, placing the same meal across multiple days and overlaying the glucose curves makes it easier to see whether the dip is a consistent pattern or a one-off. That comparison is often more useful than reviewing any single day in isolation. Download SNAQ to start comparing meal patterns alongside your glucose data.
If You Don't Have Diabetes
If you are using a CGM without a diabetes diagnosis and seeing post-meal glucose dips, the most likely explanation is normal glucose regulation. Blood glucose rises after eating and returns to baseline. A small dip slightly below your starting level is usually not a concern on its own unless it comes with symptoms like dizziness, shakiness, or confusion.
Reactive hypoglycemia can occur in people without diabetes, but it is less common. If you are seeing frequent symptomatic lows after eating, it is worth discussing with a clinician to look into the cause.
References
- American Diabetes Association. Standards of Medical Care in Diabetes. Diabetes Care, 2020. doi.org/10.2337/dc20-S011
- International Diabetes Federation. Managing Postprandial Blood Glucose. idf.org
- Jenkins DJA, et al. Effect of a low-glycemic index or a high-cereal fiber diet on type 2 diabetes. JAMA, 2002. doi.org/10.1001/jama.287.19.2414
- Surwit RS, Schneider MS, Feinglos MN. Stress and Diabetes Mellitus. Diabetes Care, 1992. doi.org/10.2337/diacare.15.10.1413
- Basu R, et al. Time Lag of Glucose From Intravascular to Interstitial Compartment in Humans. Diabetes, 2013. doi.org/10.2337/db13-1132
- Altuntas Y. Postprandial Reactive Hypoglycemia. Sisli Etfal Hastan Tip Bul, 2019. pubmed.ncbi.nlm.nih.gov/32377086