Quick answer: GMI and A1C measure glucose through completely different biological pathways: one measures interstitial glucose over the past two weeks, the other reflects red blood cells over the past three months. A gap between them is common, and often more informative than a match. Understanding why they differ can tell you which number to trust more in your specific situation.
GMI and A1C are both trying to answer the same question: how well managed is your glucose? But they do it through different biological systems, on different timescales, using different measurement methods. That's not a flaw in the design. It's why the gap between them can tell you something a single number never could.
Here are six common reasons they diverge, and what each one actually tells you.
What GMI and A1C Actually Measure
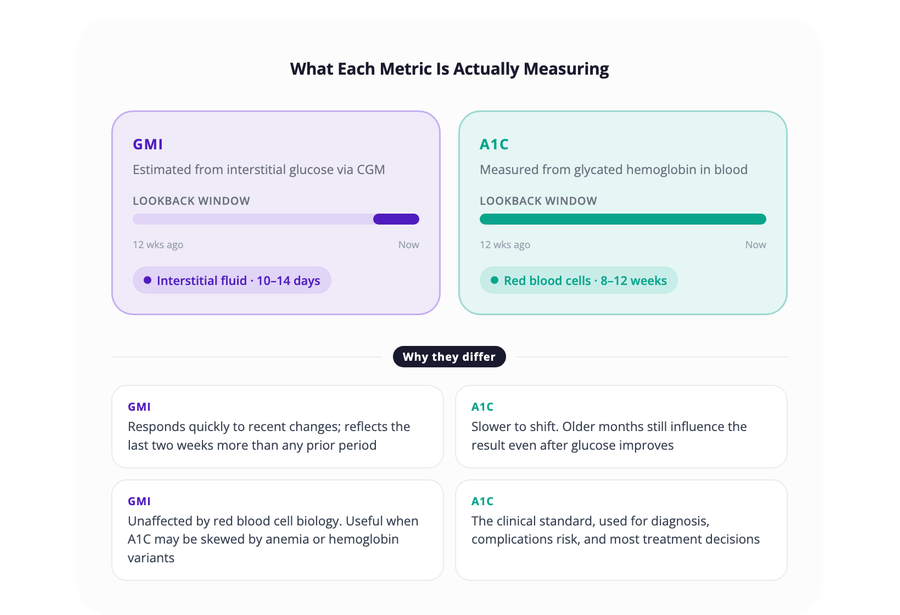
A1C measures glycated hemoglobin: the percentage of red blood cells that have glucose attached to them. Because red blood cells live for roughly three months, A1C reflects your average glucose over approximately 8 to 12 weeks.
GMI is calculated from your CGM data. It estimates what your A1C should be based on your average glucose over the past 10 to 14 days. It is a prediction, not a direct measurement. It was originally called "estimated A1C" (eA1C), but the name was changed specifically because patients and clinicians kept being confused when the estimate didn't match their lab result. The new name was chosen to signal that the two metrics are distinct, not interchangeable.
They are related, but they measure different things through different systems. That difference is where the useful information often lives.
1. Red Blood Cell Turnover Variability
A1C assumes your red blood cells last about three months. That is an average, not a constant.
Some people turn over red blood cells faster than average. Others turn them over more slowly. If your red blood cells are shorter-lived than typical, your A1C may read lower than your actual glucose exposure would predict. If they live longer, your A1C may read higher.
GMI is not affected by any of this. It uses only glucose readings from interstitial fluid, bypassing hemoglobin entirely. So if your red blood cell lifespan is unusual, whether due to anemia, hemoglobin variants, pregnancy, certain medications, or chronic kidney disease, GMI and A1C can drift apart even when your glucose is stable.
This is one of the most clinically meaningful reasons for a persistent gap. If you have a condition that affects red blood cell biology, your A1C may be systematically misleading in one direction, and GMI may be giving you a more accurate picture of what your glucose is actually doing.
2. Recent Glucose Changes
GMI reflects your most recent CGM data, usually the past 10 to 14 days. A1C reflects a weighted average of the past two to three months, with the most recent weeks carrying somewhat more influence, though still a fraction of the total.
If your glucose control improved sharply in the last few weeks, GMI will already reflect that. Your A1C is still averaging in months of older data and will take longer to catch up.
The reverse is also true. A difficult few recent weeks will show up clearly in GMI before A1C registers the change. This is not an error in either metric. It is the temporal offset that makes them complementary: GMI shows you what is happening now, A1C shows you what has happened over a longer arc.
If you changed your diet, started a new medication, or had an illness recently, this timing gap is likely doing most of the work in any mismatch you're seeing.
3. CGM Calibration and Lab Variability
CGMs measure glucose in interstitial fluid. Lab tests measure glucose bound to hemoglobin in whole blood. These are not the same thing, and the conversion between them introduces its own margin of error.
Most modern CGMs report mean absolute relative difference (MARD) values between 8% and 10%, meaning individual readings can vary from a reference blood glucose measurement by that margin. Lab A1C tests also carry variability. The same blood sample tested at two different labs can produce slightly different results depending on the equipment, testing method, and sample handling.
Small measurement differences in either direction can compound into a noticeable gap between GMI and A1C, especially when your glucose sits near a clinical threshold where small differences carry more weight in decisions. There is also a known directional bias in the GMI formula: it tends to overestimate A1C when your actual A1C is below 7.0%, and underestimate it when your A1C is above 8.0%. If your glucose consistently runs at either end of the range, this formula bias alone can account for a portion of the gap.
It is also worth knowing that clinically significant discordance (gaps of 0.5% or more between GMI and A1C) occurs in roughly one in three patients, according to research. This is not a rare edge case. It is common enough that a mismatch should be the starting point for a question, not a source of anxiety.
For a deeper look at the factors that affect CGM readings specifically, see 7 Factors That Affect Your CGM Accuracy.
4. CGM Wear Time and Data Gaps
GMI is only as reliable as the data behind it. If you wore your sensor inconsistently, had compression lows during sleep, experienced sensor errors, or had gaps in coverage, your GMI is built on an incomplete sample.
A1C does not have this limitation. It reflects every hour of the period, whether you were wearing a sensor or not.
Most CGM platforms require at least 70% sensor uptime over a 10 to 14 day window before they will generate a GMI at all. If you are below that threshold, GMI may not appear, or may be based on data that skews toward times when you were paying active attention to your glucose, which may not represent the full picture.
5. Hemoglobin Variants and Medical Conditions
Certain hemoglobin variants, including hemoglobin S (sickle cell trait), hemoglobin C, and hemoglobin E, can interfere with how accurately a given lab method measures A1C. The degree of interference depends on which test method the laboratory uses, and not all labs test for this.
Beyond hemoglobin variants, conditions including iron deficiency anemia, vitamin B12 deficiency, chronic kidney disease, and liver disease can alter red blood cell lifespan or hemoglobin glycation rates. The result is an A1C value that does not accurately reflect your actual glucose exposure, in either direction.
In these situations, GMI may give a more reliable signal because it bypasses the hemoglobin pathway entirely. That said, GMI is not a clinical replacement for A1C. Most care guidelines, insurance requirements, and medication adjustment decisions still rely on laboratory A1C as a primary marker. But when there is a persistent gap that doesn't have an obvious explanation, hemoglobin variants and these conditions are worth discussing with your care team, particularly if your lab uses an older testing method.
6. Glucose Variability Patterns
Two people can have the same average glucose but very different daily curves. One person might spend most of their time between 80 and 140 mg/dL. Another might swing between 60 and 200 mg/dL multiple times per day. Both could have similar GMI and A1C values, because both metrics reflect the average, not the shape of the curve.
High variability does not automatically cause a GMI–A1C mismatch, but it adds another reason why neither metric tells the complete story on its own. A consistent average built on a flat curve is a different physiological situation than the same average built on large swings, even if the numbers look identical on paper.
Time in Range captures what GMI and A1C cannot: what proportion of the time your glucose is actually within a healthy window. For practical strategies to improve Time in Range alongside A1C, see How to Improve Your Time-in-Range: A Practical Guide.
How to Use GMI and A1C Together
There is an active clinical conversation about how much weight GMI deserves. A 2024 perspective in Diabetes Care argued that GMI performs poorly as an A1C estimate and that reporting raw CGM mean glucose would be simpler and cause less confusion. Whether or not that view prevails, it points to something worth keeping in mind: GMI was designed as a bridge metric, not a standalone one. It is most useful when read alongside A1C and Time in Range, not instead of them.
When GMI and A1C agree closely, you have confirmation that your CGM data aligns with your lab results. When they diverge, treat the gap as a question worth investigating rather than a problem to resolve. A persistent gap in the same direction, with GMI consistently running higher or lower than A1C across multiple readings, usually reflects something real about your individual physiology: red blood cell turnover, a hemoglobin variant, or a consistent CGM calibration bias. That pattern is worth bringing to your care team.
Track both over time. The direction and consistency of the gap often matters more than any single mismatch.
When you do bring it to your care team, the conversation is more useful if you come prepared with specifics: the approximate size of the gap, whether it has been consistent across multiple A1C measurements or has shifted, and whether anything changed in the period before the mismatch appeared. A new medication, an illness, a change in CGM device, or a stretch of lower sensor wear time are all worth mentioning. That context helps your care team distinguish between a gap that reflects individual biology and one that points to a fixable measurement issue.
Separately, researchers are actively exploring personalized GMI models that account for individual biology rather than a one-size-fits-all population formula, though none have reached clinical practice yet. The direction of travel suggests the two metrics may become easier to reconcile over time.
If you use SNAQ, one practical use of the GMI trend view is comparing it against the meals and patterns from the same period. When your average glucose shifts and GMI moves with it, having meal context on the same timeline makes it easier to see what actually changed: a new breakfast routine, a reduction in evening snacks, or a stretch of more consistent meal timing. That context is what turns a number into something you can act on. Download SNAQ.
References
- American Diabetes Association. Standards of Medical Care in Diabetes, 2021. Diabetes Care, 2021.
- National Institute for Health and Care Excellence. Type 1 diabetes in adults: diagnosis and management. NICE guideline NG17, 2015.
- Battelino T, et al. Clinical targets for continuous glucose monitoring data interpretation: recommendations from the international consensus on time in range. Diabetes Care, 2019.
- Beck R, et al. Factors affecting CGM-calculated GMI. J Diabetes Sci Technol, 2017.
- Cohen RM, et al. Red blood cell lifespan and its impact on glycation. J Diabetes Sci Technol, 2010.
- Bergenstal RM, et al. The Glucose Management Indicator: Time to Change Course? Diabetes Care, 2024.