A pizza dinner looks different on a CGM than a bowl of pasta, even if the carb counts are similar. The spike might come later, last longer, or show up twice. Understanding why requires looking at the whole curve, not just one number two hours after eating.
Quick answer: A delayed spike usually means a longer tail, not random CGM noise. Mixed meals with higher fat and/or protein can shift glucose rises to three or more hours after eating. Focus on Peak, Tail and Recovery, they tell a more useful story than a single checkpoint.
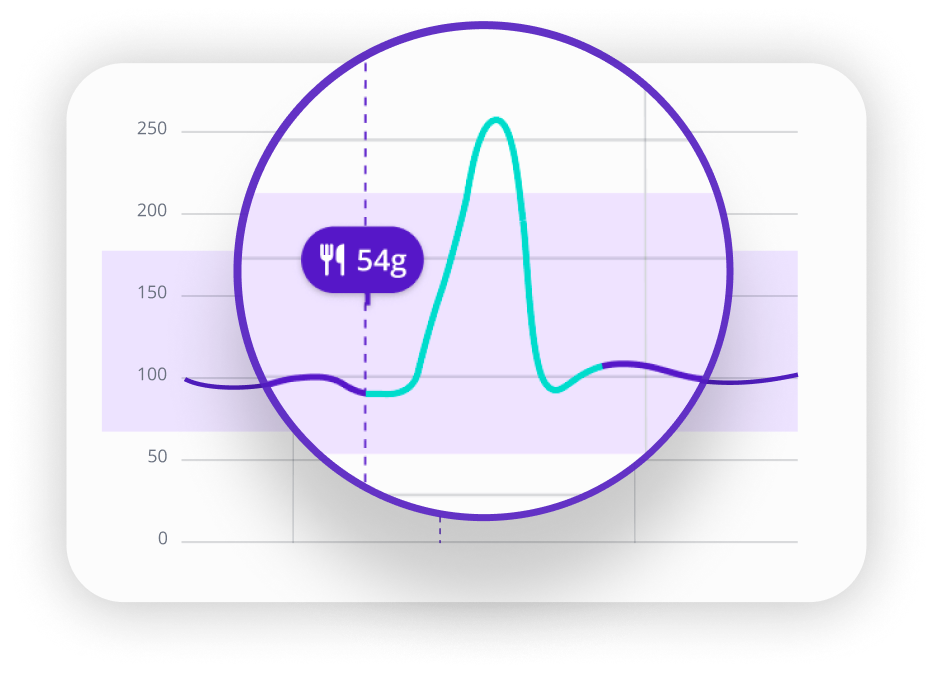
How to read a post-meal curve: peak, tail, and recovery
If you focus only on a single number at a fixed time, you miss most of what the CGM is showing you. Three labels make the shape easier to read.
Peak (time-to-peak)
How many minutes from meal start until the highest point on your CGM. This is the simplest way to describe whether a spike is "immediate" or "delayed."
Tail (late excursion)
Is your glucose still rising, or staying elevated, after about two hours? A longer tail is where most "delayed spikes" actually live, and it's also where time-in-range after meals becomes a more useful lens than a single checkpoint. Note: CGM readings run a few minutes behind blood glucose during fast changes, so treat peak timing as approximate.
Recovery (return toward baseline)
How long until you return close to your pre-meal level or your usual stable range. This is not a clinical guideline endpoint. It is a practical lens for focusing on duration, not just the peak number.
Not every meal produces a clean peak that resolves by two hours. Mixed meals can shift the highest point later, some curves look like a long hill, not a sharp spike.
Five common curve shapes
Focus on the trend, not the label. These categories help you spot patterns across similar meals.
1. Fast spike, fast recovery
Peaks early, often within one to two hours, then drops back down. Commonly linked to faster-absorbing carbs or quicker digestion.
Likely driver: Carb form (liquid, refined, or mixed) and your pre-meal glucose trend.

2. Fast spike, long tail
Peaks early, then stays elevated longer than expected. Often shows up after mixed meals with less movement afterward.
Possible reason: Fat/protein notes, portion size, and steps or activity in the two hours after eating.

3. Slow climb (late peak)
Rises gradually and peaks later. May reflect slower absorption or longer digestion, and context like a late dinner, poor sleep, or stress.
Context to check: Meal timing and a short context note (sleep, stress, activity level).

4. Double wave (second rise at 3–5 hours)
Rises, partially comes down, then rises again a few hours later. More common after meals where fat and protein are a bigger part of the plate.
Possible reason: Time of the second rise and fat/protein content of the meal.

5. Dip then rebound
A dip after eating, followed by a rebound rise. Can reflect CGM timing quirks and individual physiology. Patterns across multiple days matter more than one occurrence.
Context to check: When the dip happens, whether it repeats, and exercise or stress context.
What changes the shape: the main drivers
Carb form and absorption speed
A liquid or refined carb may produce a quicker rise than a mixed meal with fiber and fat. This is why two meals with similar carb grams can look different on a CGM. The form of the carbohydrate, not just the amount, affects how quickly glucose climbs.
Fat and protein: the late-rise effect
Protein and fat can extend the post-meal glucose window. This is best studied in type 1 diabetes, but the pattern is relevant across different types and even in people without diabetes. The result is usually a longer tail or a later peak, not a bigger early spike.
Meal timing and sleep context
Late dinners and sleep timing can shift what recovery looks like, especially if you are less active after eating. When you notice a pattern, log dinner timing and whether it was a low-movement evening. Look for repeats across similar nights.
Movement after eating
Post-meal exercise can reduce postprandial glucose excursions, and timing appears to matter. In a systematic review and meta-analysis, exercise after meals reduced excursions more than exercise before meals. An experimental study in healthy volunteers found that postprandial brisk walking reduced post-meal peaks across different meal types. A short walk after eating may soften the curve for some people, especially done soon after the meal.
Stress, illness, and day-to-day variability
Glucose patterns can shift with stress and illness. Large-scale CGM research also shows high variability in responses to the same foods, even in the same person across different days. If you notice a sudden shift, add a short context note. The goal is pattern recognition, not perfect control.
Three common scenarios
Same carbs, different shape
When the same meal produces a different curve on a different day, food usually isn't the variable. The more useful things to log are the ones that shifted: how well you slept the night before, whether the morning was stressful, and what direction your glucose was already trending before you ate. Those three non-food variables explain most day-to-day variation, and a quick context note at meal time is all it takes to start tracking them.
Lower carbs, but a later spike
If your CGM rises more at hours three to five than it did at hour one, the most useful logging action is to flag the fat and protein load of that meal, not just the carbs, and note the exact time the late rise begins. That timestamp, repeated across similar meals, is the pattern worth tracking. Over a few weeks, it becomes clear which specific meal compositions consistently push your curve later.
Up, down, then up again
A single double-wave is not necessarily a problem. But if it repeats consistently, for same meal type, same rough timing on the second rise, that pattern is worth documenting and sharing with your care team. Log the time of the first peak, the time of the second rise, and what you ate. A few consistent examples are far more useful in a clinical conversation than a vague sense that "something happens a few hours after dinner."
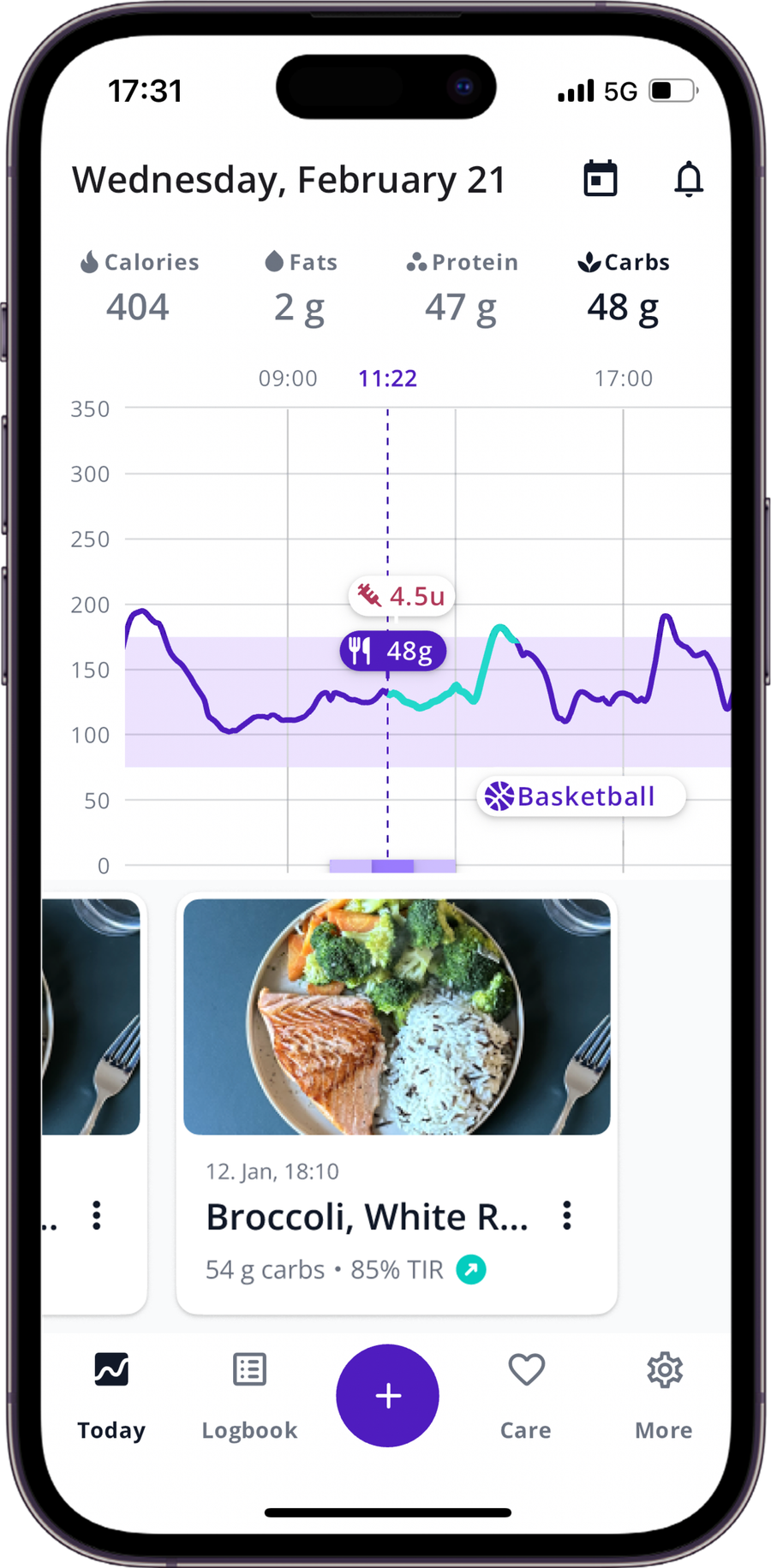
Using SNAQ to spot which meals drive a longer tail
If your goal is to understand why a meal spiked late, consistent logging is the most useful tool. Here is a simple workflow in SNAQ:
- Log the meal with accurate timing, so you can compare time-to-peak and tail across similar meals.
- The app analyses your food with AI, giving an estimate on carbs and macros.
- Connect your CGM to overlay meals on your CGM graph. You can see whether certain meal types create a longer tail or a double-wave pattern.
- Use AI Coach as an educational helper to identify and understand the pattern (peak, tail, recovery).
What to remember
The more you log, the faster patterns become obvious. One curve tells you very little; ten similar meals start to tell you something real.
Next meal: SNAQ logs meal timing, carbs, and macros automatically. You can add a context note directly in SNAQ, sleep quality, stress, or post-meal movement, so it sits alongside your glucose curve in the same view. That note, repeated across similar meals, is what turns a CGM curve into a pattern you can actually use.
The goal is not to "win" one meal. It is to build a library of patterns you can recognize.
If you want to turn your CGM curves into patterns you can actually recognize, download SNAQ on App Store or Google Play.
Frequently asked questions
Why does my blood sugar spike 3 hours after eating?
A three-hour spike is often a tail pattern, where glucose stays elevated or keeps rising after the main peak. Mixed meals with higher fat and/or protein can shift rises later, especially in people with type 1 diabetes. CGM lag can also make timing appear slightly later during fast changes.
Why does my blood sugar spike 4 hours after eating?
A four-hour rise can happen when a meal produces a longer digestion and absorption window. Research in type 1 diabetes suggests fat and protein can contribute to later post-meal excursions, sometimes in the three-to-five hour range.
When does blood sugar usually peak after a meal?
In diabetes guidance, postprandial checks are typically described as one to two hours after meal start, often near peak levels in people with diabetes. But peak timing can vary by meal, person, and day. Mixed meals can shift the highest point later.
What causes a double spike after eating?
A double-wave pattern can occur after mixed meals, where an early rise is followed by a second rise a few hours later. Small studies in pump-treated type 1 diabetes and reviews discussing fat and protein effects support this as a plausible mechanism, though results vary by person and context.
Can fat and protein delay a glucose spike?
Yes. Fat and protein can slow digestion and extend the post-meal glucose window, which often shows up as a longer tail or later rise rather than a bigger early spike. Most of the research comes from type 1 diabetes studies, but the mechanism, fat slowing gastric emptying, protein triggering a glucose response, is not unique to T1D. The pattern is worth tracking regardless of whether you have diabetes.
Does a CGM show glucose later than a fingerstick?
CGMs measure interstitial glucose, so a short delay versus blood glucose is expected. One analysis reports an average delay of around nine to ten minutes. Lag can matter more during rapid changes, like fast rises after meals or during exercise.
What matters more: the peak number or return to baseline?
Often, the duration and tail of the excursion are more informative than a single peak number. A practical return-to-baseline lens helps you focus on how long the meal affected your glucose, which is often more useful than chasing the exact highest point.
Is it normal for blood sugar to rise 2 hours after eating?
A rise at two hours can be part of a typical post-meal response, especially in diabetes, where postprandial checks are commonly framed at one to two hours after meal start. But some meals have a longer tail, which can keep glucose elevated beyond two hours.
References
1. American Diabetes Association. 6. Glycemic Goals, Hypoglycemia, and Hyperglycemic Crises: Standards of Care in Diabetes-2026. Diabetes Care (supplement). 2026.
2. Battelino T, Danne T, Bergenstal RM, et al. Clinical Targets for Continuous Glucose Monitoring Data Interpretation: Recommendations From the International Consensus on Time in Range. Diabetes Care. 2019;42(8):1593-1603.
3. Smart CE, Evans M, O'Connell SM, et al. Both Dietary Protein and Fat Increase Postprandial Glucose Excursions in Children With Type 1 Diabetes, and the Effect Is Additive. Diabetes Care. 2013.
4. Bell KJ, Smart CE, Steil GM, Brand-Miller JC, King B, Wolpert HA. The Role of Dietary Protein and Fat in Glycaemic Control in Type 1 Diabetes: Implications for Intensive Diabetes Management. 2015.
5. Pankowska E, Szypowska A, Lipka M, Szpotanska M, Blazik M, Groele L. Does the fat-protein meal increase postprandial glucose level in type 1 diabetes patients on insulin pump: the conclusion of a randomized study. 2012.
6. Schmelzeisen-Redeker G, Schoemaker M, Kirchsteiger H, Freckmann G, Heinemann L, del Re L. Time Delay of CGM Sensors: Relevance, Causes, and Countermeasures. J Diabetes Sci Technol. 2015.
7. Zaharieva DP, Turksoy K, McGaugh SM, et al. Lag Time Remains with Newer Real-Time Continuous Glucose Monitoring Technology During Aerobic Exercise in Adults Living with Type 1 Diabetes. Diabetes Technol Ther. 2019.
8. Zeevi D, Korem T, Zmora N, et al. Personalized Nutrition by Prediction of Glycemic Responses. Cell. 2015.
9. Engeroff T, et al. After Dinner Rest a While, After Supper Walk a Mile? A Systematic Review with Meta-analysis on the Acute Postprandial Glycaemic Response to Exercise Before and After Meals. Sports Medicine. 2023.
10. Bellini A, Nicolo A, Bazzucchi I, Sacchetti M. The Effects of Postprandial Walking on the Glucose Response after Meals with Different Characteristics. Nutrients. 2022.
12. Fendt SM, et al. Continuous Glucose Profiles in Healthy Subjects under Everyday Life Conditions and after Different Meals. 2009.
13. Zhou J, et al. Reference Values for Continuous Glucose Monitoring in Chinese Subjects. 2009.
14. Blonde L, Umpierrez GE, Reddy SS, et al. American Association of Clinical Endocrinology Clinical Practice Guideline: Developing a Diabetes Mellitus Comprehensive Care Plan - 2022 Update. 2022.
15. International Diabetes Federation. International Diabetes Federation guideline for management of postmeal glucose: a review of recommendations. 2009.
The SNAQ website does not contain medical advice. The contents of this website, such as text, graphics, images and other material are intended for informational and educational purposes only and not for the purpose of rendering medical advice. The contents of this website are not intended to substitute for professional medical advice, diagnosis or treatment. Please consult your healthcare professional for personalized medical advice.